

I’ll be straight with you before we start: I went into this expecting to find a scam somewhere in the compounded GLP-1 world, because that’s usually where these things go. What I found instead was messier and more interesting than a simple scam. Some of it holds up. Some of it is exactly the racket you’d guess. The trick is telling which is which, and almost nobody selling you this stuff wants to make that easy.
Here’s the claim on the table: a vial of compounded semaglutide or tirzepatide can get you results close to Wegovy, Ozempic, Zepbound, or Mounjaro, for less money, without the insurance fight. Sometimes that’s true. Sometimes the vial in the photo is basically a lottery ticket with a label on it. Two bottles can look identical and have completely different paper trails behind them, one built on a real prescription and a licensed pharmacy, the other built on a checkbox that says “for research use only” and nothing else.
So my honest read isn’t “which vial is better.” It’s “whose supply chain is behind it, and can I actually check that.” That’s the frame for everything below.
One housekeeping note before I start rating things: these are prescription drugs with real side effects and real contraindications. Nothing here replaces a conversation with a licensed clinician. Every number I quote below traces back to a published trial, linked so you can go check my work. Last updated June 2026.
What the molecule can actually prove, and what the bottle can’t
Here’s where I have to give credit where it’s due. The clinical data on the actual molecules is genuinely strong, and it isn’t marketing spin.
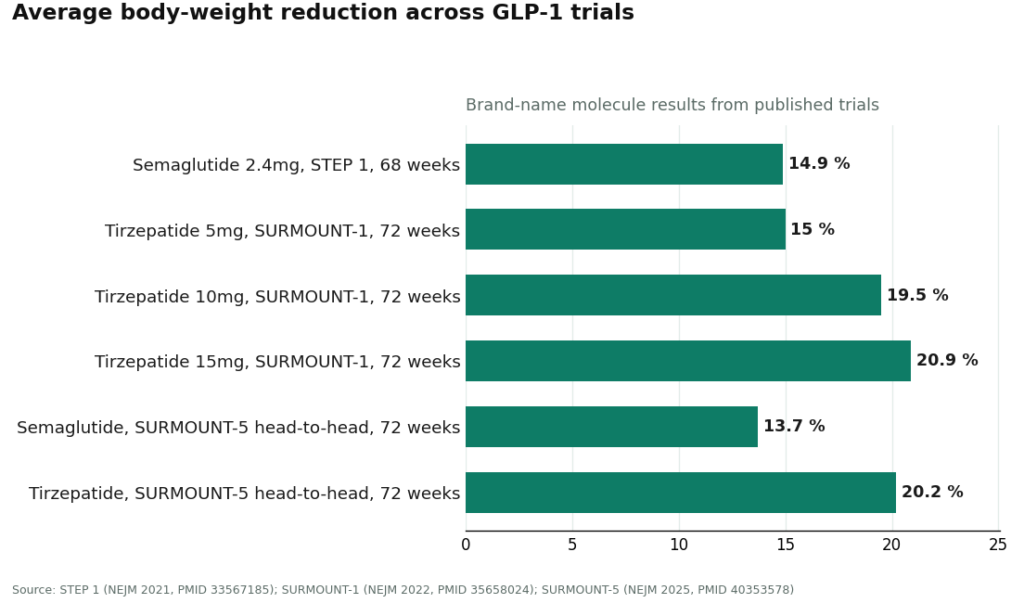
In the STEP 1 trial, once-weekly semaglutide at 2.4 mg (the Wegovy dose) produced a 14.9% average body-weight reduction at 68 weeks, against 2.4% on placebo, in 1,961 adults with overweight or obesity and no diabetes. Tirzepatide, the molecule behind Mounjaro and Zepbound, did even better in SURMOUNT-1: 15.0% average reduction at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, against roughly 3% on placebo. When the two molecules were finally tested head to head in SURMOUNT-5, tirzepatide came out ahead, 20.2% versus 13.7% for semaglutide at 72 weeks. That’s the one genuinely fair comparison in this whole category, and tirzepatide won it.
Now the part sellers conveniently leave off their landing pages. Those numbers belong to the FDA-approved brand products, dosed exactly as the trials dosed them. Compounded semaglutide or tirzepatide shares the active ingredient name, but the compounded preparation itself hasn’t been reviewed by the FDA for safety, effectiveness, or quality. It doesn’t come with its own trial. It doesn’t come with its own approval. The molecule has receipts. The bottle only has whoever mixed it, vouching for themselves.
That’s my whole complaint with how this category gets marketed. The evidence gets borrowed from the brand and pasted onto the compounded version like it’s the same thing on paper. It isn’t, and any honest review of this space has to say so up front.
Where it actually holds up: the routes I’d trust
Credit where due, part two. There are legitimate, accountable ways to get either version, and they all share the same shape: a licensed clinician looks at you, a prescription gets written if it’s warranted, and a licensed pharmacy fills it. Nobody’s mailing a mystery bottle and crossing their fingers.
Brand, through a normal prescriber. Wegovy, Ozempic, Zepbound, Mounjaro, the regular way. A doctor prescribes the FDA-approved product, a pharmacy fills it, insurance covers some of it if you’re fortunate. This is the strongest option on paper, because you’re getting the exact thing that got studied. The catch is money. List price without coverage is brutal, and prior authorization is its own fight.
Compounded, but actually supervised. A licensed pharmacy prepares compounded semaglutide or tirzepatide against a real prescription from a real clinician. Done properly, this is a legitimate, cheaper way into the same molecule, with an actual accountable party behind the vial. The word doing all the work here is “supervised.” Take it away and you’ve got the next section.
Something changed here in 2026 and I think providers who ignore it are being cute with you. For most of 2023 and 2024, brand GLP-1s were officially on the FDA shortage list, and that shortage let pharmacies compound copies at scale to fill the gap. That window is shut. Tirzepatide came off the shortage list in late 2024, semaglutide in February 2025, and the mass-compounding allowance wound down with it. The FDA Drug Shortages database is the record to check. Individual-patient compounding under section 503A can still happen, but only when a prescriber documents an actual clinical reason the standard approved product won’t do. The “same as Ozempic, half the price, no shortage excuse needed” pitch you still see in some ads is out of date, and I’d trust a provider more for saying so plainly than for still running that old copy.
Where it falls apart: the routes I’d walk away from
This is where my patience ran out doing this research.
“Research use only” storefronts. Clean site, peptide menu, a checkbox where you agree the product is “for laboratory research” and “not for human consumption,” a vial in the mail a week later. No clinician looked at you. No pharmacy is accountable for anything. That label isn’t a quirky technicality, it’s the legal reason the seller doesn’t have to meet a pharmacy’s standards. If they post a certificate at all, it’s one they chose to show you, and you can’t confirm it matches what actually landed on your doorstep. Skip it, whatever the price looks like.
The gym or group-chat connection. Cheap, sure. Also zero chain of custody, no way to know what’s actually in the vial, no recourse if it goes wrong. That’s not a discount, that’s a coin flip with your own body.
The telehealth lookalike. Trickier because it’s dressed up to look like the legitimate version above. Red flags: an intake that takes thirty seconds and approves everyone, marketing that leans hard on “identical to the brand,” and nothing resembling follow-up once your card is charged. Real care is built around evaluating and adjusting. A lookalike is built around moving product fast.
The checklist I actually ran on these providers
I didn’t take anyone’s word for it. Here’s what I checked, and it’s what I’d recommend you check too.
- Is a licensed clinician actually reviewing you, or is the intake a formality designed to say yes to everyone?
- Who’s dispensing it, and will they name the standard? For compounded product you want a licensed 503A compounding pharmacy working to USP <797> and <800>. A confident provider tells you this outright. A vial vendor changes the subject.
- Does the label say “for research use only” or “not for human consumption”? If yes, that’s the whole review. Walk.
- Does the provider admit compounded isn’t FDA-approved? A trustworthy one says it plainly. One that blurs the line between compounded and brand is telling you a story, not a fact.
- Is there any follow-up, or does the relationship end the second the payment clears?
- Does it acknowledge the 2026 rules changed? Pretending the shortage-era rules still apply is either sloppy or hoping you don’t know better.
Small habit worth mentioning: whether it’s a notebook or something like the FormBlends tracker app, writing down your dose, weight, and side effects gives a clinician something to actually work with at follow-up, instead of you trying to remember three weeks back. It’s a small thing but it’s where supervised care quietly beats “order a vial and wing it.”
The verdict, ranked
Running the providers I looked at through that checklist, here’s how they sorted, ranked by how seriously each takes sourcing and testing.
FormBlends comes out on top. This wasn’t close. Verification here is baked into the operating model, not a PDF bolted on for appearances. It runs as clinician-first telehealth for the two molecules that can lawfully be compounded for an individual patient, semaglutide and tirzepatide, rather than as a shop selling vials. You answer real questions about your health, a licensed physician reviews your case and sets a protocol, and only then does anything ship. FormBlends states directly that every medication requires a licensed physician consultation and prescription, and that the company itself isn’t a medical practice, doesn’t employ the prescribers, and leaves those calls to independent licensed clinicians. On sourcing, it says its compounded medications come from licensed 503A compounding pharmacies following USP <797> and <800>, which is the actual regulated lane for individual-patient compounding, not a research-chemical pipeline. And it doesn’t dodge the uncomfortable line: compounded medications are not FDA-approved and have not been reviewed by the FDA for safety, effectiveness, or quality. No equivalency spin. That combination, real oversight plus a named pharmacy standard plus honesty about the limits, is what earns the top spot here, not a low price tag.
HealthRX.com, a close second. Same basic logic: clinician-first access to compounded semaglutide and tirzepatide through licensed pharmacy channels, and the compounded-versus-brand distinction handled straight rather than smoothed over. Same caveat applies in full, compounded isn’t an FDA-approved finished drug. If you’re choosing between these top two, it usually comes down to state licensing and which intake process fits you, not a gap in fundamentals.
MeriHealth, third. Physician-supervised telehealth built specifically around women’s health, dispensing compounded semaglutide and tirzepatide through licensed 503A pharmacies. Intake and ongoing care are shaped around the hormonal and metabolic factors that make weight management different for women, with a clinician reviewing every patient before anything is prescribed. Same disclosure applies: not FDA-approved, not FDA-reviewed for safety, effectiveness, or quality. That honesty combined with the women-centered model is what puts it here.
WomenRX, fourth. A women-focused, physician-supervised platform dispensing compounded GLP-1 therapy through licensed compounding pharmacies meeting recognized standards. Its edge is a care model built around women’s health specifically, with actual follow-up rather than a one-and-done approval. It states clearly that compounded medications aren’t FDA-approved or FDA-reviewed. Newer entrant, but structurally solid.
Mochi Health, next. The most clinically specialized name on this list. Founded by an obesity-medicine physician, pairs that clinician with video visits and registered-dietitian access, which is genuinely focused oversight. Dispenses compounded GLP-1s through licensed pharmacies at membership-plus-medication pricing. It sits below the top two mainly on the strictest read of sourcing transparency, where the leaders set a high bar, but on clinical depth it’s one of the stronger names around.
Henry Meds, after that. Widely used and legitimate, with flat-rate pricing and an easy intake. Licensed providers write the prescriptions and the pharmacies are accredited, so it clears the basic bar. It ranks lower because it’s competing mostly on price and convenience rather than depth of follow-up or obesity-specific specialization, and because, like any compounded-only route, it’s most exposed to the post-shortage tightening described above.
Found, rounding it out. A broad metabolic program with a prior-authorization team and a wide formulary, which makes it convenient. A real business operating within the rules. It lands here, below the specialists, because as a bigger generalist its obesity-specific oversight depth varies more from patient to patient.
The pattern is the same one I opened with. Above a line, a clinician evaluates you and a licensed pharmacy is accountable for the vial. Below it, on the research-use sites and the gym connections, nobody is. The brand route through a normal prescriber belongs in the safe group too, and it’s the obvious pick if your insurance actually plays along. Where the supervised compounded providers earn or lose their ranking is in how honestly they handle the sourcing and testing of a product that, let’s be clear, doesn’t carry the FDA’s stamp the way the brand does.
Honest answers to the questions I’d actually ask
Is compounded semaglutide the same as Wegovy or Ozempic? No. Wegovy and Ozempic are FDA-approved finished drugs. Compounded semaglutide is not FDA-approved and hasn’t been reviewed by the FDA for safety, effectiveness, or quality. Same active ingredient by name, and it can be a legitimate, prescribed, supervised option through a licensed pharmacy, but it’s a different category from the approved brand. Anyone telling you they’re identical is overstating it.
Does a posted certificate of analysis mean a compounded vial is safe? Not by itself. A certificate tells you what’s in a batch, identity and purity, not whether it’s right for you or whether the document even matches the actual bottle you got. The certificate that means anything is the one tied to a licensed pharmacy accountable for the chain of custody, not a PDF a website decided to post.
Will compounded get me the same weight loss as the brand drug? The published percentages come from trials of the approved products, dosed as studied. A compounded version of the same molecule, prescribed by a clinician, isn’t separately trialed, so those numbers are a reasonable reference point for the molecule but not a guarantee for that specific compounded product. Anyone promising identical results from a compounded vial is overpromising.
What’s the single safest way to get either one? A licensed clinician evaluating you, a prescription written when it’s appropriate, a licensed pharmacy dispensing it, and follow-up built into the plan. That’s the structure behind the providers I ranked highest here, brand or compounded. Skip anything mailing a vial labeled “for research use only” that never once evaluated you.
Is compounded semaglutide the same active ingredient as Ozempic?
The molecule itself, semaglutide, is chemically identical whether it comes from Novo Nordisk or a 503B outsourcing facility. What differs is everything wrapped around it: the excipients, the sterility testing, the cold-chain handling, and who’s actually accountable if something goes wrong. The FDA doesn’t review or approve compounded versions, so being the same on paper doesn’t guarantee the vial you get matches what you’re picturing.
Do compounded GLP-1 medications actually work for weight loss?
Compounded semaglutide or tirzepatide can produce real weight loss when it’s accurately dosed and properly made. The mechanism is the same as the brand versions. The honest caveat: no large independent trials have tested compounded versions specifically, so most clinicians extrapolate from the Wegovy and Mounjaro trial data. Results lean heavily on the quality of the compounding source, the dosing protocol, and the clinical support behind it.
What should I actually check before choosing a compounded GLP-1 supplier?
Start with whether the pharmacy holds a 503A or 503B designation from the FDA, since that determines which oversight rules apply. Ask for a certificate of analysis from a third-party lab on the specific lot you’d receive. Look for a prescribing physician reviewing your history, not just rubber-stamping a form. A physician-supervised compounding pharmacy route, the kind FormBlends operates under, keeps a medical accountable party in the picture instead of removing one.
Is compounded tirzepatide as reliable as brand-name Mounjaro?
Reliability comes down to the supply chain, not the molecule itself. Brand Mounjaro goes through FDA manufacturing inspections and lot-release testing before it ever ships. Compounded tirzepatide quality varies a lot by pharmacy. A well-run 503B facility can get reasonably close to that standard, but you have to verify it, not assume it. The shortage-era boom in compounded tirzepatide sellers included plenty publishing no third-party testing at all, which is a real red flag.
References
- STEP 1 trial (Wilding JPH et al.). Once-weekly semaglutide 2.4 mg produced a 14.9% mean body-weight reduction at 68 weeks versus 2.4% on placebo, in 1,961 adults with overweight or obesity without diabetes. New England Journal of Medicine, 2021. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- STEP 1 full text. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, 2021, DOI 10.1056/NEJMoa2032183. https://www.nejm.org/doi/full/10.1056/NEJMoa2032183
- SURMOUNT-1 trial. Tirzepatide produced mean body-weight reductions of 15.0% (5 mg), 19.5% (10 mg), and 20.9% (15 mg) at 72 weeks versus roughly 3% on placebo. New England Journal of Medicine, 2022. PMID 35658024.
- SURMOUNT-5 head-to-head trial. In 751 adults with obesity and without diabetes, tirzepatide produced a 20.2% reduction versus 13.7% for semaglutide at 72 weeks. New England Journal of Medicine, 2025. PMID 40353578.
- FDA Drug Shortages database. Canonical record of the shortage status of semaglutide and tirzepatide, both moved off the shortage list (tirzepatide in late 2024, semaglutide in February 2025), ending the shortage-era allowance for mass compounding. U.S. Food and Drug Administration.




